KNOW MORE ABOUT PCL RECONSTRUCTION
- Home
- KNOW MORE ABOUT PCL RECONSTRUCTION

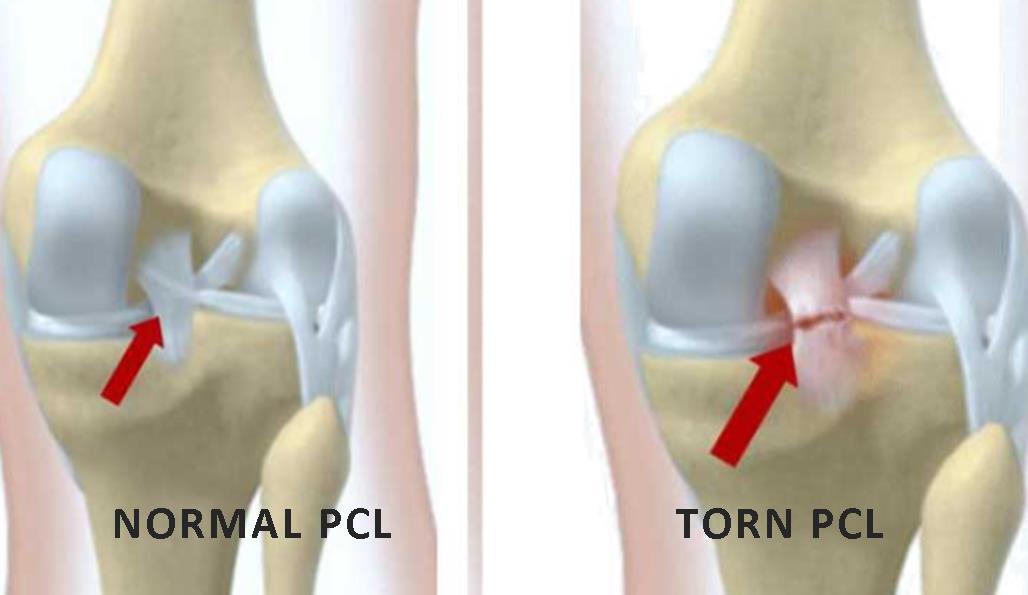
What is a PCL Reconstruction:
The PCL Reconstruction is the toughest ligament of the knee joint, it is damaged few often considering for about 5-35% of all knee fractures. In knee structure, the PCL Reconstruction has located on middle and back areas. PCL also connects the thighbone to the shinbone.
What is PCL reconstruction:
In every posterior cruciate ligament (PCL) reconstruction procedure requires grafting. Basic PCL reconstruction procedure grafting on torn or damaged ligaments with hamstring tissue. If PCL has major damage then doctor use multiple grafting procedures.
most of all methods utilize uniquely outlined bolts allotting strong infatuation the grafting matter inside bone holes penetrated into the knee. The operation is usually taken a day before the complete surgical procedure.
The function of the PCL:
Restrict the backward migration of the knee.
Turning behind on itself, Restrict forceful expansion of the knee joint,
Supports and stable the knee on spin moves and work as a primary axis of the orbit of knee
PCL Tear Symptoms:
Having Slow movement of the knee.
Due to pain while up-down the stairs.
having problems, in turn, and twist the knee.
Due to Feeling internal knee pain.
Having swelling and instability in the knee.
Causes of PCL injury:
The PCL can tear :
1. your knee ligament tibia is bumped hard just under the knee.
2. When you slip and fall on a twisted knee.
Treatment for PCL Reconstruction:
Treatment depends on the amount or infected area of your damaged part. In maximum cases, surgery doesn’t require.
A physical Therapy:
A physical surgeon can guide you some activities that will help to make your knee harder and enhance its balance and stability. A doctor may prescribed brace or crutches for your knee during your recovery.
Surgery:
If your PCL has fully damaged or injured and having more pain in the knee, Therefore An orthopedic doctor recommended PCL reconstruction surgery. The PCL will not recover automatic and it is not feasible to reconstruct a ripped one. So an alternative tissue needs to used to replace it.
In addition, PCL rehabilitation is normally done under common analgesic (asleep) to assure the tissues enclosing the joint are sufficiently comfortable to handle the method. The local anesthetic is penetrated around the knee at the end of the surgery to help low hurting and pain.So, Four cuts around 5mm-20mm in length, are done around the knee to set the camera and surgical tools into the joint, pick the graft and move it into the knee. Probably PCL restoration takes between 45 minutes and 2 hours.
Recovery after PCL tear surgery:
Especially After the surgery patients have to start operated knee flexion at 0-90° on day one.
Use crutches and braces on an affected knee for first 4-6 months.
Do RICE activity daily: Rest, Ice, compression and elevation, it helps to reduce swelling and pain.
Take regularly prescribed medicine by your doctor.
Protect the operated knee.
Don’t drive any vehicle until your doctor not recommend to drive.
Do daily exercise prescribed by your surgeon.
In conclusion, If you are having any question about the PCL reconstruction please contact knee arthroscopy surgeon- Dr. Harish Talreja .
Call Us Today for Consultations
Feel free to pay us a visit. You won’t regret it for sure.