AVN HIP TREATMENT IN JAIPUR
- Home
- AVN HIP TREATMENT IN JAIPUR

What is Avascular Necrosis of the Hip
Bones are living tissue, and just like any other living tissue, they rely on blood arteries to keep them alive. Most live tissues contain several blood arteries that enter the tissue from various directions. There may be a backup blood supply coming in from a different route, so if one blood artery is broken, it may not create difficulties. However, just a few blood arteries deliver blood into certain joints in the body. The hip is one of these joints. This paper will explain what happens when the hip’s blood supply is disrupted, resulting in a condition known as avascular necrosis (AVN).
Osteonecrosis (which means “bone death“) is another name for this illness.One of the real ball-and-socket joints in the body is the hip joint. The acetabulum, or hip socket, is a deep cup that surrounds the ball of the upper thigh bone. The femur is the thigh bone itself, while the femoral head is the ball on the end. The ball and socket configuration allow for a wide range of motion in the hip, which is necessary for daily tasks like walking, squatting, and climbing stairs. The hip is surrounded by thick buttock and thigh muscles in the rear and front.
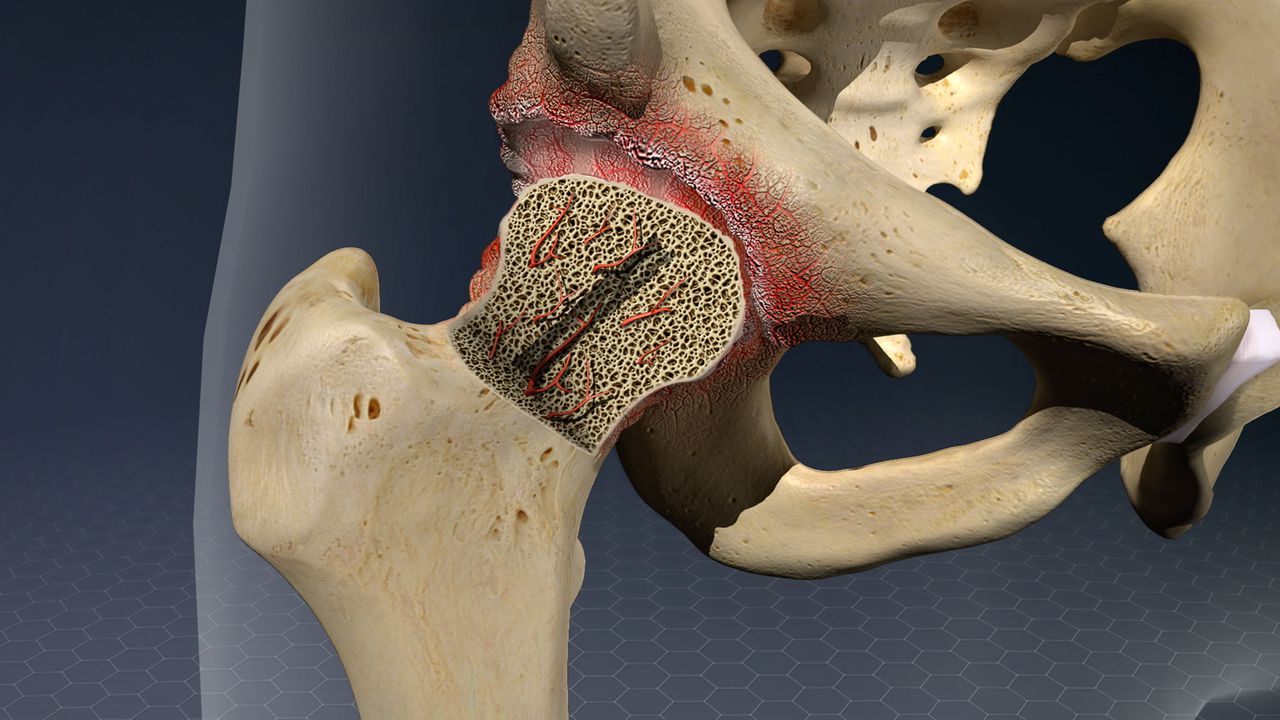
Cause of Avascular Necrosis of the Hip
When the blood supply to the femoral head is cut off, osteonecrosis of the hip occurs. The bone in the head of the femur dies and progressively collapses if it is not properly nourished. As a result, the articular cartilage that covers the hip bones degrades, resulting in painful arthritis. The bone at the head of the femur progressively dies due to osteonecrosis.
Risk Factors
Although the origin of a shortage of blood flow is not always recognized, there are a number of risk factors that might make someone more prone to acquire the disease, let us know more about them before you go for AVN Hip Treatment in jaipur. Steroid drugs are used to treat a variety of disorders, including asthma, rheumatoid arthritis, and systemic lupus erythematosus. Although it is unclear why these drugs might cause osteonecrosis, evidence suggests there is a link between the condition and long-term steroid usage.
Symptoms of Avascular Necrosis of the Hip
Osteonecrosis manifests itself in phases in Avascular necrosis Hip Treatment. The most common symptom is hip discomfort. A dull discomfort or throbbing pain in the groin or buttock area may result. Standing and putting weight on the afflicted hip will become more difficult as the condition advances, and manipulating the hip joint will be uncomfortable.
The time it takes for the disease to develop through these phases might range from months to years. It’s critical to detect this condition early since research shows that early treatment leads to better outcomes. Osteonecrosis can develop from a healthy hip (Stage I) to the femoral head collapsing (Stage IV).
Doctor Examination for the Treatment of Hip Pain
Your doctor will check your hip after discussing your symptoms and medical history to determine which motions give you discomfort. Osteonecrosis can be detected by increased discomfort during particular motions.
Imaging Exams: The following imaging studies may be used to confirm a diagnosis of avascular necrosis of the hip:
X-rays: Scans of dense structures, such as bone, produce images. X-rays are used to determine whether and how much the femoral head bone has collapsed. Scans using magnetic resonance imaging (MRI). An MRI scan can detect early abnormalities in the bone that may not be seen on an x-ray. These scans are utilized to determine the extent to which the illness has impacted the bone. An MRI may reveal early osteonecrosis that has not yet shown itself as a symptom.
AVN Hip Treatment in Jaipur
Although nonsurgical treatments such as medications or crutches can relieve pain and slow the progression of the disease, surgical treatments are the most effective. Hip preservation operations are appropriate for patients with osteonecrosis that is detected early (prior to femoral head collapse).
Decompression of the Core
This technique entails drilling one or bigger holes into the femoral head in order to alleviate pressure on the bone and provide routes for new blood vessels to supply the hip’s afflicted regions.To help regenerate healthy bone and support cartilage at the hip joint, core decompression is frequently combined with bone grafting. A bone graft is healthy bone tissue that is transferred to a required part of the body.There are several bone transplant alternatives accessible today. Harvesting additional bone from one region of your body and grafting it to another portion of your body is the normal procedure. An autograft is a name for this sort of graft.
What are the Hip Replacement Preoperative Instructions?
There are various components to an orthopedic surgeon’s examination.
Medical background: Your orthopedic surgeon will ask questions about your overall health and the amount of your hip discomfort, as well as how it impacts your ability to do daily tasks.
Examination of the body: The mobility, strength, and alignment of the hips will be evaluated.
X-rays: These photos aid in determining the amount of your hip’s injury or deformity.
Another testing is being conducted: Other tests, such as a magnetic resonance imaging (MRI) scan, may be required in some cases to evaluate the quality of your hip’s bone and soft tissues.
Before you go to the hospital, learn as much as you can about the procedure you’ll be having. Your hospital should offer written or video documentation. Maintain as much activity as possible. It will help you recuperate if you strengthen the muscles around your hip.
Get Best AVN Hip Treatment in Jaipur
Dr. Harish Talreja is Jaipur’s most renowned and experienced orthopedic surgeon, specializing in knee, hip, and joint replacement surgery. He is the Best Hip Replacement Surgeon in Jaipur.
You may feel confident that whatever condition you have, will be treated
We’ll be able to directly address it and help you improve your health.
He is a doctor who is qualified and well-trained
Our physician is highly knowledgeable and well-trained and it’s quite adaptable.
Dr. Harish Talreja is capable of completing any assignment that is placed in front of him.
He only utilizes environmentally friendly products.
Give us a call now and book your appointment with us today for the best results.
Call Us Today for Consultations
Feel free to pay us a visit. You won’t regret it for sure.