MENISCUS TEAR: CAUSES, SYMPTOMS AND TREATMENT
- Home
- MENISCUS TEAR: CAUSES, SYMPTOMS AND TREATMENT

Overview of a meniscus tear
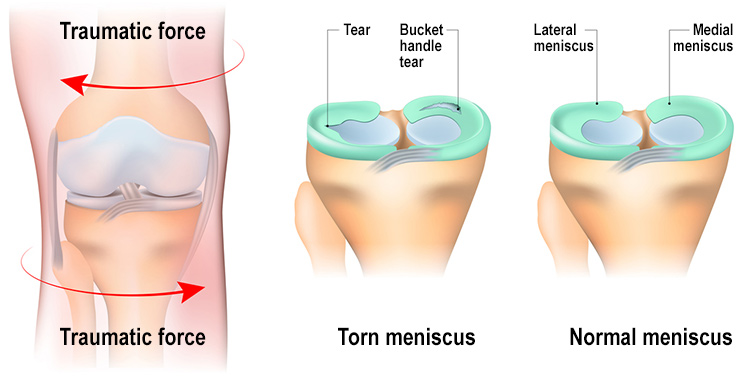
There are a plenty of knees damage or injuries, a meniscus tear is also severe and Painful. Normally, it’s very common problem happens in athletes and common person. In fact, a meniscus tear is one of the most often happening cartilage offenses of the knee. what is meniscus? The meniscus is a part of cartilage between the thigh bone(Femur) and shinbone(tibia ) that provides a cushion and supports the joint. There is two menisci cushion in each knee joint.The meniscus cushion defends the knee bones from wear and tear problem. But all it needs is a good turning of the knee joint to tear the meniscus.
The cushion can be destroyed or damaged while doing motions or activity that put weight, force, and pressure or rotate the knee joint frequently. Like a football player playing football in a field and sudden take hard tackle or a sudden shaft of the sports can causes a meniscus damaged.
Causes of a meniscus tear:
Meniscus tears are normal in playing sports like basketball as well as nonplaying sports person needing jumping and sudden movements such as volleyball and football. A meniscus tear can occur when a person shifts direction quickly while working, and often happen at the same time as other knee damage, like an ACL tear damage. An immediate shaft or rotation, deep crouching, or heavy lifting can begin to injury.Some sports need sudden or immediate rotate the knee and stop running may put stress on the knee and this creates a higher risk of meniscus tear injury like:
Football
basketball
volleyball
tennis
So, Meniscus tears are unusual in older athletes or person. More than 40% of people have this problem in older age.
Symptoms of a meniscus tear
You can feel a click or pop sound in the knee. Maximum people can walk and do the movement in the injured knee. Many athletes keep playing with a Meniscus tear. Over 2 to 4 days, the affected knee will constantly grow more hardness and swelling.
Then, you may feel
Having pain in knee especially when you touch that area
Due to swelling and redness in an affected area
Having difficulty in moving the knee
Lack of motion area of the knee.
Knee locking.
Having difficulty in bending your knee
Sensing your affected knee “goes out”.
Surgical Treatment
Knee surgery is one of the most common procedures. In Meniscus, a tiny camera enters into a small hole. This helps to view clear part of the inside of the knee. Your orthopedic doctor injects miniature surgical implements by other holes to lick or fix the tear.Following are two methods to improve your meniscus tear
1. Partial Meniscectomy method- In this method, the affected meniscus muscle is scraped away. 2. Meniscus repair method- Sometimes the damage meniscus tears can be fixed by stitching the split parts mutually. Whether a tear can be successfully performed with replacement depends on the type of infection, as well as the overall the injured meniscus. The meniscus need heal back mutually, the recovery time for a healing take much time than from a meniscectomy.
Recovery at home
Once the operation was conducted successfully, and healing the meniscus is completely heal then your physician will guide for rehabilitation exercises. Daily exercise also helps in knee movement and power. You have to start exercises to increase your knee limit of motion.
Use crutches or braces
Use ice on an operated knee to reduce swelling
compress your knee with an elastic bandage to controlling swelling
Elevate your affected knee with a pillow to increase healing tissues
Take the medicine regularly.
Use stretching exercise to help reduce stress to your knee
Especially Avoid jumping and running for start 3 to 4 months after surgery
Results
Long-term outlook after surgery With the good determination of treatment, your operated knee can have the movement and capacity it had before the surgery. If a meniscus tear is healed by nonsurgical treatment, the rate of improvement depends on the area of the damaged.
As a result, If you are having any type of pain, please contact best knee specialist doctor.
Call Us Today for Consultations
Feel free to pay us a visit. You won’t regret it for sure.