PATELLAR DISLOCATION
- Home
- PATELLAR DISLOCATION

What is PATELLAR DISLOCATION
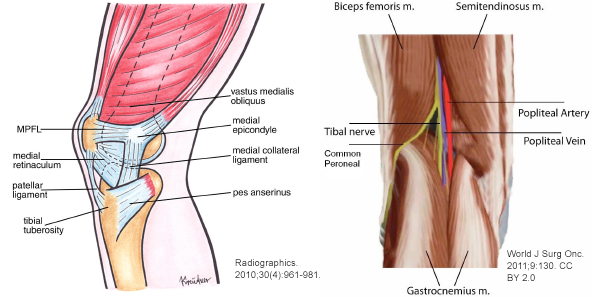
In a healthy knee, your patella is located within a trench at the base of the thigh bone(femur). Therefore, Relocation of kneecap from its usual arrangement will cause Patellar dislocation.The most general direction for a kneecap to break or fracture apparently. If this occurs, the tissues and ligaments on the interior of the knee shift overstretched and injured.
SYMPTOMS OF PATELLAR DISLOCATION:
1. Visible adaptation of the kneecap (Knee gives out). 2. Sufferers who have disturbed patella or kneecap dislocation will tell that “my kneecap shifted out of place”. 3. Having pain when weight bearing and doing the normal activity of the knee. 4. Due to Swelling and tenderness around your kneecap. 5. Feels instability of the quadriceps muscles of the knee. 6. The affected knee will normally be sensitive to touch or having pain.
WHAT CAUSES PATELLA DISLOCATION?
The major cause of Patellar dislocation injury due to an accident or sudden twisting or direct hit on the knee.There are several causes of having patellar dislocation or kneecap dislocated.
If the knee joint conflicts with heavy things with big force, injury to the joint can cause the patella dislocation.
When a sportsman is running speedily in one direction and instantly change the direction of legs. Therefore, knee joint feels pressure. In this case, the pressure is too much and can harm the kneecap.
Females have a high risk of patellar(kneecap) dislocation than males. Therefore, this danger occurs because, females manage to have wider hips bones, causing the thigh bones bend within and joint the knee at further of an angle.
Peoples who have thin or week leg tissues or an inequality in the power of their individual legs may put unneeded stress on their knee joint, this stress on a knee is raising the hazard of patellar dislocation.
A person who is abnormally tall may have an extended risk of the patellar disorder.
Having beforehand experienced a kneecap disorder or another traumatic damage that has reduced the knee joint may improve the likelihood of transferring a kneecap dislocation.
People who are seriously higher weight or fat are more expected to bear a kneecap disorder, and a dislocation can happen even without the bearing of traumatic damage or excess strength. Therefore, It is known as a low-velocity patellar dislocation, the knee is destroyed due to the weight of bringing the body and disturbs the joint alignment.
TREATMENT OF DISLOCATED KNEECAPS
Treatment for dislocated knee will differ depending on the cruelty of the damage.
Nonsurgical Treatment for a Patellar Dislocation
In most cases of patellar dislocation, various nonsurgical medication choices will try before prescribed direct surgery to fix the kneecap. Common nonsurgical procedures are:
The first acknowledgment treatment for the injury, a patient instructed to apply RICE therapy, rest, ice, compress and elevate on the kneecap.
Non-steroidal anti-inflammatory remedies may prescribe to approach reduce both the pain and swelling.
Sometimes the patellar or kneecap will shift back into position on its individual as the leg move. If it has not done, a surgeon tries to fix the kneecap manually until it’s in the exact position.
A patient may use crutches or braces to reduce stress on the knee joint and patella.
Surgery:
If the dislocated kneecap is particularly difficult or may have also produced destruction to the neighboring ligaments, and muscles, surgery require to fix the kneecap or replacement other compositions. Common operations for patellar dislocation are:
Arthroscopic surgery: This type of operations includes entering a small camera into the knee joint and using a predicted picture to fix what damage has been created in the knee by displacement.
Reconstructive surgery: The Reconstructive surgery will typically be initiated after arthroscopic surgery has already completed. Especially In this surgery doctor’s do fixing or repairing spoiled cartilage, Fix a critically disturbed kneecap or fixing damaged ligaments and muscles.
HOW TO PREVENT RECURRENT PATELLA DISLOCATIONS?
After patellar dislocation surgery, the chance of recurrence is approximately 50% without taking rehabilitation and healing. Patella dislocation occurs frequently then it causes risk of re-injury.
For this reason, it is very necessary to consider your injury or problems with your physiotherapist. They will guide you the best treatment plan for increase healing and rehabilitation of your knee. Also, they ensure that you receive sufficient rehabilitation to greatly decrease your risk of continuing knee problems.
As a result, For more information please contact to Dr. Harish Talreja – A Knee arthroscopic doctor in Jaipur
Call Us Today for Consultations
Feel free to pay us a visit. You won’t regret it for sure.