ACL RECONSTRUCTION
- Home
- ACL RECONSTRUCTION

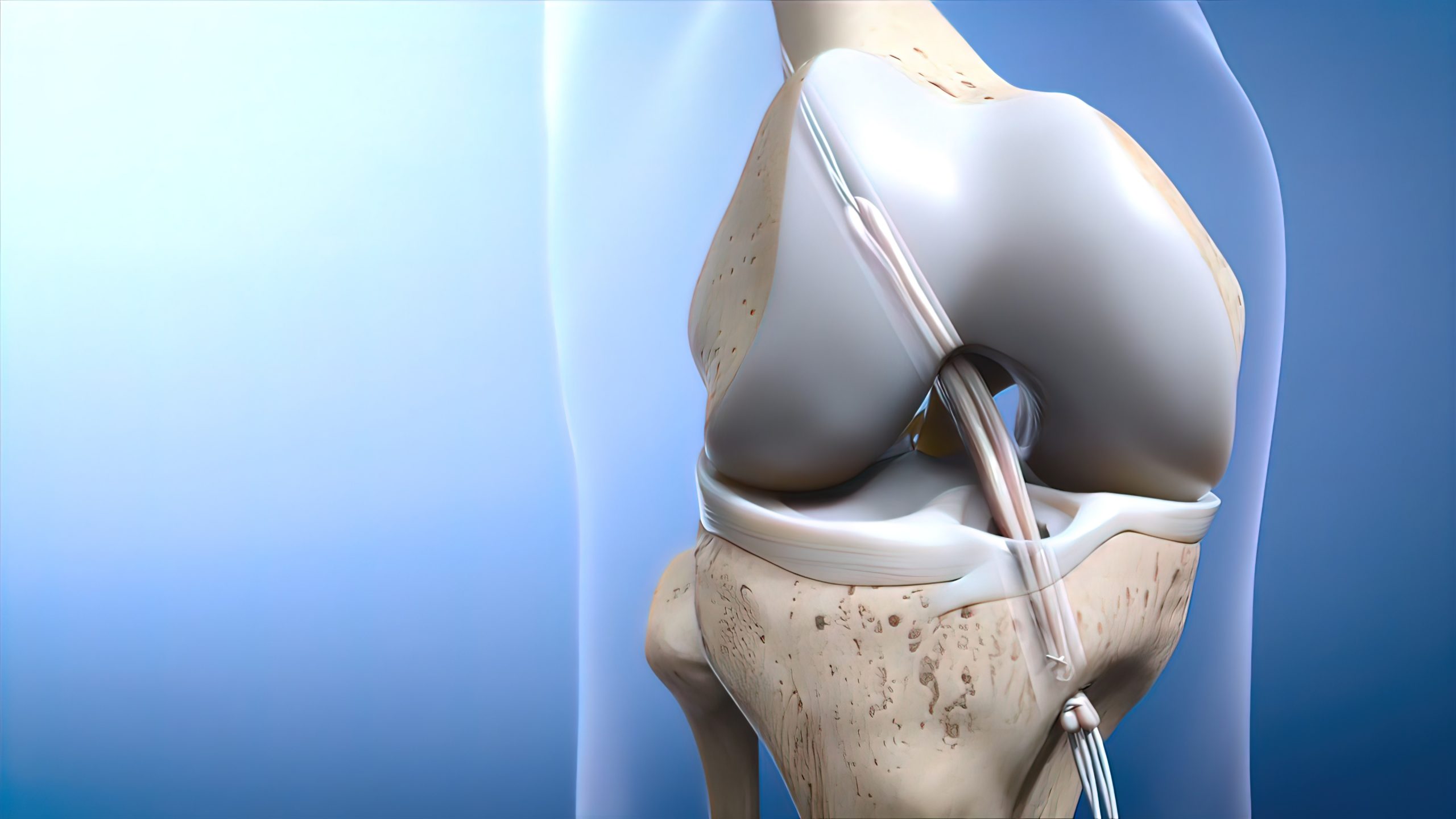
Anterior cruciate ligament: ACL Reconstruction
ACL reconstruction is common in people who play sports games. The anterior cruciate ligament is a band of tissue within the knee.The knee joint bone structure is created by the tibia, patella, and femur. The anterior cruciate is the 4th main ligament in the knee that attach the tibia to the femur.In normal language, ACL is a knee ligament that joins the above leg bone with the lower leg bone.When your anterior cruciate ligament is good or healthy, it helps to maintain the joint between the femur and tibia. Therefore, ACL helps to keep your knee strong and stable. If ACL gets injured or damaged from an accident or sudden movement, you may have difficulty in placing weight or pressure on your knee, playing sports, walking, or seating.
What causes an ACL injury?
Your ACL can be damaged if your knee joint is bent behind or twisting side by side. The risk of damage is larger if more than one of these actions happens at the same time.An ACL damage usually happens while playing sports games. The injury can happen when your leg is located on the earth and an unexpected strength beats your knee while your leg is vertical or lightly twisted. This can appear when you are shifting direction quickly, reducing speed when running, or landing from a height. This type of damage is prevalent in soccer, skiing, and other sports games that having many go and stop activities, weaving or jumping. Dropping off stairs are another likely problems with having an ACL injury.
Symptoms
Due to the Sensing, Feeling or catching a pop or knock in the knee joint at the time of damage.
Have swelling around the damaged knee within the first few time of the damage.
Having Pain or hurting on the knee and back of the knee.
Damaged restricted knee movement because of hurting inside or swelling.
After serious damage, you will seem to stop everything you are doing because of the hurting, but you may be capable to walk.
Long-term results or outcomes:
After improvement and recovery, you will be ready to raise your operated shoulder to just up shoulder height and twist the elbow to touch the top of your head. ACL RECONSTRUCTION surgery gives excellent effort in relief due to the pain and sufferer satisfaction is very high.
In addition, If you are looking for a ACL RECONSTRUCTION surgery doctor, Please contact Dr. Harish Talreja, the best ACL RECONSTRUCTION doctor in Jaipur.
Who needs ACL reconstruction?
If you have split or torn your ACL, your orthopedic surgeon is likely to recommend an ACL reconstruction if your knee is unstable or unhealthy.
In the past sufferers played a lot of sports games and want to go back to playing sports.
To have another injury to your knee.
Choices to have ACL reconstruction:?
Some sufferers from an ACL damaged may not require surgery to improve it. You may have physiotherapy treatment, exercises, and a joined knee lining to give knee support. Your orthopedic doctor may recommend this type of therapy if:
your knee should be stable.
you have a small part of torn in your ligament, rather than fully torn it.
your age is 65+ or above and don’t play a sports game.
What Happens During the Operation?
Your orthopedic surgeon will replace the torn ligament with new tissue(Tendon) from your knee. The purpose is to prepare your knee shelter and stability again and give it the full extent of movement and motion.
Recover from an ACL reconstruction surgery:
ACL reconstruction normally needs 5-6 months to get a full improvement.
Don’t do too much walking, seating and standing.
Use a walker or crutches for a walk for two weeks after surgery.
Don’t align vertically with your operated leg and don’t bend it to 90 degrees after 2-3 weeks of surgery.
Don’t drive any vehicle until your surgeon recommended it.
As a result, If you wanted to take any advice about the ACL Reconstruction, please contact to best Knee arthroscopy doctor, Dr. Harish Talreja.
Call Us Today for Consultations
Feel free to pay us a visit. You won’t regret it for sure.